1. INTRODUCTION
The transition from a pandemic to an endemic phase of COVID-19 marks a significant shift in the global public health paradigm. This evolution has profound implications for Thailand, where the virus’s endemicity introduces new challenges and necessitates strategic adaptations in response to its mutating strains. This situation has a significant impact on working-age individuals, highlighting the need for innovative approaches to prevent and manage information post-pandemic. Because COVID-19 is now endemic, there is a need for ongoing and flexible methods to share and use health information. In this situation, having current information about COVID-19 is very important for daily life (Kim & Oh, 2023). Working-age individuals actively seek different sources of information to stay updated and adapt to the changing landscape of the disease. This includes not only seeking answers to specific questions, but also utilizing acquired knowledge to tailor responses and reduce risks associated with the regular presence of the virus.
The cognitive process of information perception (INF) plays a pivotal role in this adaptive strategy, encompassing the selection, comprehension, interpretation, and retention of relevant information. This process is inherently influenced by individuals’ prior experiences (Clements, 2020). In the current context, the veracity and dependability of information gain unprecedented importance, as misinformation or reliance on unreliable sources can precipitate inappropriate responses, increased anxiety, and potentially hazardous behaviors (Ali et al., 2020). Given the dense population of Bangkok and its metropolitan area, along with its history of significant COVID-19 outbreaks, this region emerges as a critical focal point for examining these dynamics. By focusing on the working-age demographic within this densely populated urban setting, valuable insights can be gleaned into the interplay between INF and self-protective behaviors during the endemic phase of COVID-19.
Previous research has primarily focused on the immediate impact of knowledge and information on the pandemic, addressing short-term responses and crisis management (Duplaga, 2022; Ounsaneha et al., 2023; Pothisa et al., 2022; Sánchez-Arenas et al., 2021). There is a notable gap in understanding how INF influences ongoing preventive behaviors (PVT) in the endemic phase of COVID-19. Therefore, the purpose of this study is to examine how people’s perceptions of information relate to their PVT. This understanding not only benefits the working-age population and broader community in adapting to the new normal, but also provides strategic guidance for stakeholders in the medical, public health, and media sectors. Such insights are particularly pertinent for devising tailored information dissemination strategies and public health interventions, thereby facilitating effective management of the endemic stage of COVID-19 in Thailand and analogous contexts.
2. BACKGROUND AND LITERATURE REVIEW
2.1. Information Perception
Perception is a fundamental aspect of human behavior that begins with and is based on knowledge obtained through sensory experiences. Human behavior primarily manifests through the process of organizing, selecting, and interpreting stimuli or other information, which is influenced by how a person perceives their surroundings. This perception is then translated into thoughts, emotions, decisions, and behaviors. Each person’s perspective of the same circumstances may result in different interpretations due to the different perceptions that arise from individual values (Gibson, 1991; Greenberg & Baron, 2003; Schiffman & Kanuk, 2007). Ultimately, perception enables individuals to respond to their needs, obtain information that supports decision-making, retention, and interpretation, and make efficient use of the perceived knowledge in varied contexts.
INF is a vital process in understanding the events of the world, incorporating an individual’s knowledge, abilities, experiences, and perspectives. The selection of information involves a series of steps, leading to varied perceptions among individuals. Although the perception process is unique to each person, it generally consists of three stages, which are exposure, interpretation, and retention (Assael, 2004; Roediger, 1990; Schermerhorn et al., 2002). Information exposure, the initial stage, involves opening oneself to stimuli and selecting specific information aligned with preferences, often through various media such as daily COVID-19 infection reports. After exposure, individuals interpret the received information, by thinking, analyzing, and evaluating its credibility, influenced by personal perspectives and experiences. For instance, interpreting COVID-19 pandemic information might require analyzing it through personal beliefs. Finally, individuals retain information, storing it for future reference, which enhances awareness and influences future behaviors. For example, members of the working-age population may retain COVID-19 prevention measures for an extended period. While the INF process is dynamic and individualized, these three stages provide a general framework for understanding how individuals select, interpret, and retain information, ultimately shaping their unique perspectives and responses.
2.2. Preventive Behavior of COVID-19
The COVID-19 disease has become endemic in Thailand, with frequent and widespread occurrences of infections. Members of the working-age population must possess knowledge about proper self-protection methods for themselves and their families to ensure safety from infection. The working-age population, both in Thailand and internationally, exhibits information behaviors categorized into four dimensions: hygiene, prevention of spread, maintaining good health, and digital way of life (Suanrueang et al., 2022). These dimensions guide individuals in adapting diverse aspects of their lives, fostering awareness, and giving emphasis to the severity of the disease’s impact on health.
2.2.1. Hygiene
Hygiene includes the observable sanitary practices that reflect people’s desire to avoid infection by engaging in various unsafe behavioral practices (Suanrueang et al., 2022). People’s knowledge significantly influences self-healthcare behaviors, encompassing rigorous cleaning practices at home using soap. This extends to the sanitization of frequently touched surfaces such as handrails and doorknobs (Hayashi et al., 2022). In response to coughing or sneezing, individuals adhere to the use of tissues to cover their nose or mouth, followed by thorough handwashing. Handwashing is essential for preventing disease transmission (Alzoubi et al., 2020; Hernández-García & Giménez-Júlvez, 2020). It involves washing hands with soap and water for at least 30 seconds, or using alcohol-based hand sanitizers as an alternative (Chavis & Ganesh, 2020). Individuals also exhibit behaviors such as avoiding unnecessary touching, refraining from sharing personal items, and employing designated utensils when dining with others. Additionally, it is recommended to avoid consuming raw or undercooked animal products due to food hygiene, as good food safety practices can prevent transmission through food (World Health Organization, 2020).
2.2.2. Prevention of Spread
Preventing the spread of COVID-19 involves immediate isolation and seeking medical attention at local health-promoting sub-district hospitals or nearby clinics upon showing symptoms, or after exposure to someone with symptoms (Güner et al., 2020). In case of illness, home isolation is advised to prevent close contact with others, encompassing avoidance of face-touching, hugging, or proximity to colleagues or those in the vicinity (Ju et al., 2021). The continuous tracking of COVID-19 information through various channels contributes to heightened awareness, emphasizing the severity of the disease and the importance of preventative measures (Anwar et al., 2020). The adaptability of the working-age population in various aspects reflects their understanding of the COVID-19 situation, showcasing adjustments in physical, role-related, and interdependence aspects (Scheibe et al., 2022). This demonstrates their ability to handle information effectively and make informed decisions for proper self-care and safety.
2.2.3. Maintaining Good Health
In maintaining overall health, various working-age groups are observed to adopt methods that enhance both their physical and mental well-being. These efforts aim to strengthen immunity while adhering to strict measures to control the spread of COVID-19, aligning with their new lifestyle (Khalifa et al., 2021). Noteworthy health maintenance techniques include consuming nutritious food, which is essential. A well-rounded meal has been related to healthier wellness, stronger immune systems, and a lower likelihood of infectious and chronic illnesses in people (Nuertey et al., 2022; World Health Organization, 2024). It was shown that people are more likely to adhere to safe dining guidelines if they have a positive attitude about food safety and strong family norms (Soon et al., 2021). Furthermore, engaging in physical exercise emerges as a pivotal element in equipping and reinforcing the immune system’s resilience against COVID-19 (da Silveira et al., 2021; Fernández-Lázaro et al., 2020). Moderate physical activity was shown to be beneficial in modulating the immune system, reducing inflammation, and improving mental health during the pandemic (Hagiu, 2021). Quality sleep and sufficient rest are crucial factors affected by the prolonged COVID-19 pandemic (Varma et al., 2021). Poor sleep was linked to higher levels of anxiety, depression, and stress, emphasizing the need for public health interventions focused on sleep to improve mental health during the pandemic. Nonetheless, prioritizing adequate and effective rest has positive effects on both physical and mental health, contributing to higher immunity and reducing the risk of infection.
2.2.4. Digital Way of Life
The adoption of a digital lifestyle acknowledges that COVID-19 has become an endemic disease. Measures have been implemented to gather information related to the surveillance of various respiratory system disorders, ensuring a comprehensive understanding of the situation and preparedness for disease treatment (Alghamdi & Alghamdi, 2022). In cases of mild symptoms, individuals can opt for general medication to alleviate the condition. Self-care practices contribute to heightened awareness, fostering self-care and prevention. Adhering to guidelines post-contact or following proximity with symptomatic individuals is essential to prevent severe illness and hospitalization. The working-age population has demonstrated commendable compliance with government recommendations, following disease control protocols during travel, maintaining strict social distancing measures, and minimizing contact with others or shared items. Nevertheless, public health initiatives should persist in providing clear knowledge and guidelines at the individual, community, and institutional levels, adapting to evolving circumstances (Karijo et al., 2021). People have significantly adapted to the new lifestyle, relying on technology for communication in various aspects, including public health, work, education, economics, and social interactions (Dubois et al., 2022). This behavioral shift, influenced by the current circumstances, highlights the role of technology in shaping contemporary life and becoming a familiar aspect of people’s lives in the present era.
2.3. The Relationship Between Information Perception and Preventive Behaviors of COVID-19
The persistent acquisition of information pertaining to COVID-19 has been pivotal in shaping self-protective behaviors, aiming to enhance safety and reduce infection risks. The working-age demographic, in particular, values acquiring knowledge on self-health protection and perceives potential risks, thereby fostering motivation for preventive actions. Trust in public health communications emerges as a critical factor, with individuals displaying higher trust levels more likely to encourage adopting measures such as social distancing and meticulous hygiene practices (Ali et al., 2020; Fridman et al., 2020). This underscores the importance of accurate and reliable information dissemination in ensuring public compliance with health advisories. The role of digital platforms and social media in public perception and behavior towards COVID-19 preventive measures has been highlighted, with studies showing their capability to both positively and negatively impact public adherence to health guidelines (Wong et al., 2021). The advent of misinformation on these platforms necessitates a critical evaluation of information campaigns and underscores the importance of digital literacy. Furthermore, the psychological aspects of information processing, including emotional responses to health information, have been shown to significantly influence PVT (Okada et al., 2023).
Consistent exposure to information provides a comparative advantage in healthcare, enhancing individuals’ abilities to manage their well-being. Informed individuals are more proficient in making appropriate decisions concerning self-protection. Recognizing the benefits of self-protection leads to heightened motivation for practicing such behaviors. Proactively managing health conditions assists in planning effective disease prevention strategies, leading to improved health and a strengthened immune system. The working-age population’s awareness of the disease’s severity influences changes in health behavior, necessitating lifestyle adjustments, especially for those in Bangkok and the metropolitan area facing heightened infection risks. This underscores the need for evolving public health initiatives to maintain positive behavioral shifts, emphasizing the integration of informed decision-making, collective responsibility, and technological advancement for a resilient health-conscious society amidst COVID-19.
3. RESEARCH HYPOTHESES
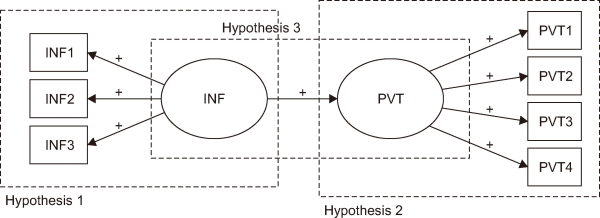
Examining the causal relationship between INF and PVT began with exploring correlation patterns among observed variables. Confirmatory factor analysis (CFA) was then utilized to validate the measurement models for each latent variable. Based on the research framework in Fig. 1, hypotheses were developed as following:
H1: INF explains a set of dependent variables comprising information exposure, interpretation, and information retention.
H2: PVT explains a set of dependent variables comprising hygiene, prevention of spread, maintaining good health, and digital way of life.
H3: INF influences PVT.

Hypotheses between information perception and preventive behavior of COVID-19. INF, information perception; INF1, information exposure; INF2, interpretation; INF3, information retention; PVT, preventive behavior; PVT1, hygiene; PVT2, prevention of spread; PVT3, maintaining good health; PVT4, digital way of life.
4. METHODOLOGY
A cross-sectional study was conducted in Thailand, focusing on working-aged individuals aged 18 to 59, comprising a total population of 10,872,100 residing in Bangkok and its surrounding metropolitan area (National Statistical Office of Thailand, 2021). The metropolitan area includes Nakhon Pathom, Nonthaburi, Pathum Thani, Samut Prakan, and Samut Sakhon provinces. The sample size was 421 individuals, which exceeds the minimum indicated in Krejcie and Morgan (1970) determining a sample size table. A convenience sampling method was used to recruit participants. An online structured questionnaire was provided using Google Forms and distributed via social media to citizen groups in each province, aiming to accurately represent demographic diversity. To collect data for this study, an online survey was undertaken from January to February 2023. This study has been certified as conforming to human research ethics by the Human Research Ethics Committees of the University (code SWUEC/E/G-197/2022).
4.1. Instrument
The research tool was a questionnaire divided into four sections: The first section included the respondents’ demographic and general information, the second section comprised INF related information, the third section contained PVT of COVID-19, and the last section included an open-ended question for additional suggestions. Five-point Likert scales ranging from 1 to 5 were used to rate each question in Section 2 and Section 3, where 5=highest, 4=high, 3=moderate, 2=low, and 1=lowest.
4.2. Validity and Reliability
The questionnaire was evaluated by three experts to check the qualification by calculating Index of Item Objective Congruence (IOC). The IOC results ranged from 0.67 to 1.00. The survey questionnaire was then adjusted according to the experts’ recommendations. Next, reliability testing was validated from gathering 42 data sets using Cronbach’s alpha as a measure of consistency, and determining how closely related a set of items are as a group. The Cronbach’s alpha for each construct was higher than the recommended level at 0.70 (Cortina, 1993). The values ranged from 0.744 to 0.920, indicating accepted reliability of the research measurement tool. Table 1 presents the results of good convergent reliability.

Reliability statistics
4.3. Data Analysis
The researchers initially analyzed the collected data using descriptive statistics to understand basic sample characteristics and respondent demographics. Mean and standard deviation calculations were employed to assess INF and PVT against COVID-19. Structural equation modeling (SEM) was then applied to explore the relationship between these variables among working-age individuals in the Bangkok and metropolitan area. Pearson’s correlation coefficient was utilized to quantify associations. Additionally, Bartlett’s test of sphericity and Kaiser-Meyer-Olkin (KMO) were used to evaluate variable appropriateness, and CFA was conducted to assess questionnaire validity within the AMOS version 21.0 (IBM Corp., Armonk, NY, USA). Finally, the causal model was adjusted to ensure its fit with the empirical data, depicting the relationships between INF and PVT against COVID-19.
5. RESULTS
5.1. Descriptive Statistics
Table 2 demonstrates the demographic profiles of the respondents. Out of 421 respondents, 295 (70.1%) worked in Bangkok and 126 (29.9%) worked in the metropolitan area. Regarding sex, 228 (54.2%) were male and 193 (45.8%) were female. Regarding the age group, 48 (11.4%) were aged 18-24 years, 102 (24.2%) were aged 25-31, 55 (13.1%) were aged 32-38, 83 (19.7%) were aged 39-45, 57 (13.5%) were aged 46-52, and 76 (18.1%) were aged 53-59. At the time the data was collected, 206 (48.9%) had received at least four vaccine dosages, 143 (34.0%) had received three dosages, 63 (15.0%) received two dosages, 3 (0.7%) received one dosage, and 6 (1.4%) had never received the vaccine. From 421 respondents, 264 (62.7%) had been previously diagnosed with COVID-19.
Respondents’ demographic information
According to a preliminary summary of INF channels presented in Table 3, the majority of participants (78.1%) obtain information through Facebook, followed by television (72.0%) and personal sources such as friends and family (56.3%). Analysis of Table 4 revealed that participants demonstrated a high level of INF regarding COVID-19, both overall and in each component. The highest mean value for information exposure was observed in perceiving COVID-19 from various channels such as social media, television, and radio ( ˉx=4.28). In the area of information interpretation, participants demonstrated a strong understanding of how to wash their hands correctly ( ˉx=4.45), and information retention indicated that with knowledge and experience, people can safely protect themselves against COVID-19 ( ˉx=4.36). Furthermore, the outcomes of PVT indicated very high levels overall ( ˉx=4.21), whereas prevention of spread behavior had the highest mean value ( ˉx=4.27).
Channels of information perception
Information perception of COVID-19
5.2. Model Verification
Table 5 shows the mean and standard deviation of each observed variable. The proposed model was initially evaluated by correlation analysis. Table 6 shows the correlation matrix of all observed variables. The statistically significance level of 0.01 implied high correlations of the variables. The highest value was the correlation between interpretation (INF2) and information retention (INF3) (r=0.771), and the lowest value was the correlation between information exposure (INF1) and digital way of life (PVT4) (r=0.442).
Descriptive statistics of latent variables
Correlation matrix
Preliminarily, KMO was used to examine the strength of the partial correlation and the Bartlett’s test of sphericity was used to analyze the factorability of the data. The value of KMO was 0.873, which implied sampling adequacy, and the chi-square was 1,801.084. From Bartlett’s test of sphericity, degree of freedom was 21 and the p-value was 0.000, which is less than the significance level of 0.001. This indicated the positive correlations of the variables. Therefore, the data can be used to conduct CFA to verify factor structures of (1) INF as shown in Table 7, and (2) PVT as shown in Table 8.
Confirmatory factor analysis of INF (information perception)
Confirmatory factor analysis of PVT (preventive behavior)
The measurement model of INF factor indicated the statistics as follows: χ2=0.005, df=1, relative χ2=0.005, p=0.946, root mean square error of approximation (RMSEA)=0.000, root mean square residual (RMR)=0.000, goodness of fit index (GFI)=1.000, normed fit index (NFI)=1.000, Tucker-Lewis index (TLI)=1.005, and comparative fit index (CFI)=1.000. It implied that INF was measured from information exposure (INF1), interpretation (INF2), and information retention (INF3).
The measurement model of PVT factor indicated the statistics as follows: χ2=1.628, df=1, relative χ2=1.628, p=0.202, RMSEA=0.039, RMR=0.002, GFI=0.998, NFI=0.998, TLI=0.996, and CFI=0.999. It inferred that PVT was found in hygiene (PVT1), prevention of spread (PVT2), maintaining good health (PVT3), and digital way of life (PVT4).
5.3. Findings of the Proposed Model
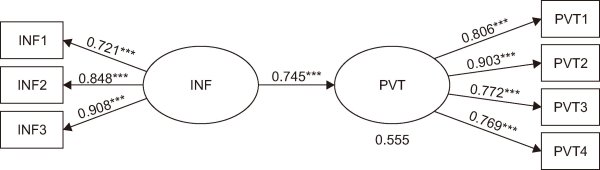
Fig. 2 illustrates the causal relationship between INF and PVT, analyzed using a SEM. The analysis shown in Table 9 confirms the construct validity of the measurement model, as all the fitness indexes meet the required thresholds. The relative chi-square (chi-square/df) was 1.043, achieving the threshold of less than 3.0. The likelihood ratio (p-value) was greater than 0.05, which indicated the validation of the measurement model and good fitness with empirical data. GFI was 0.993 and the CFI was 1.000, both of which achieved the threshold of greater than 0.90. RMSEA was 0.010, which achieved the threshold of less than 0.08.

Structural equation model between information perception and preventive behavior of COVID-19. χ2=10.434, df=10, relative χ2=1.043, p=0.403, RMSEA=0.010, RMR=0.005, GFI=0.993, NFI=0.994, TLI=0.999, CFI=1.000. INF, information perception; INF1, information exposure; INF2, interpretation; INF3, information retention; PVT, preventive behavior; PVT1, hygiene; PVT2, prevention of spread; PVT3, maintaining good health; PVT4, digital way of life; RMSEA, root mean square error of approximation; RMR, root mean square residual; GFI, goodness of fit index; NFI, normed fit index; TLI, Tucker-Lewis index; CFI, comparative fit index. ***p<0.001.
Fitness indexes of measurement model
The results of the SEM in Table 10 confirmed that INF explained a set of dependent variables comprising information exposure (βINF→INF1=0.721), interpretation (βINF→INF2=0.848), and information retention (βINF→INF3=0.908). PVT explained a set of dependent variables comprising hygiene (βPVT→PVT1=0.806), prevention of spread (βPVT→PVT2=0.903), maintaining good health (βPVT→PVT3=0.772), and digital way of life (βPVT→PVT4=0.769). Therefore, hypotheses H1 and H2 were confirmed. Finally, INF (βINF→PVT=0.745) was a significant predictor of PVT to explain 55.5% of its variance. This supported hypothesis H3.
Research findings
6. DISCUSSION
This study empirically tested the causal relationship between INF and PVT regarding COVID-19. The results revealed significance in the CFA and showed that the model was suitable for the investigation’s purpose. The findings led to the inference that the two factors chosen, INF and PVT, summarized the evidence of observed variables sought in the survey. The dependent variable of the model was the PVT of COVID-19 (PVT), and the independent variable was the INF. PVT of participants regarding COVID-19 consisted of hygiene (PVT1), prevention of spread (PVT2), maintaining good health (PVT3), and digital way of life (PVT4). The factor of INF comprised three items: information exposure (INF1), interpretation (INF2), and information retention (INF3).
INF significantly influenced PVT (β=0.745, p<0.001). This was supported by theories in earlier research. Ample evidence showed that people make decisions based on perceived information (Riva et al., 2015). Thus, INF demonstrated the level of individual health literacy. Perceived information in terms of severity and susceptibility reinforces PVT (Nazione et al., 2021). Understanding health information and the contexts in which they occur would lead to appropriate behaviors in order to achieve healthy routines and disease prevention (Rayani et al., 2021).
In addition, following the onset of COVID-19, the health practices and PVT of Thai people have undergone changes to adapt to the new normal, including practices such as hand hygiene, mask-wearing, social distancing, maintaining good health, and utilizing digital transactions to prevent virus exposure. These changes reflect the PVT relevant to COVID-19, which include hygiene, prevention of virus spread, health maintenance, and the integration of digital practices into daily life (Suanrueang et al., 2022). The first component of PVT was hygiene: hand hygiene, food hygiene, and hygienic masks have been basic protection recommendations for COVID-19 prevention (Alzyood et al., 2020; Finger et al., 2021). This approach can mitigate the exposure to infection transmission (Jantunen, 2022). The second component was prevention of spread. Even with widespread vaccine adoption, other protective behaviors, e.g., distancing, should be done in parallel to mitigate the risk of COVID-19 (Hall et al., 2023). Next, activities to maintain good health, such as exercise, sleep quality, and relaxation, promoted a healthy immune system. The last component of COVID-19 PVT was digital way of life, such as online activities. This approach can reduce physical contact and transmission of the virus. Among the variables of PVT, the prevention of spread (PVT2) had the highest factor loading at 0.903.
Furthermore, the components of INF include information exposure, interpretation, and information retention. The process initially begins with exposure, as individuals tend to select information that reinforces existing attitudes (Liao & Fu, 2013). Subsequently, information interpretation involves accessing various relevant sources to address knowledge gaps (Sangrar et al., 2021). This step entails identifying subjects, patterns, or connections within the data and using critical thinking, analysis, and evaluation to draw conclusions or make judgments, ultimately leading to a deeper understanding of COVID-19 phenomena. During crises, interpretation relies heavily on trust in information, sources, and public authorities (Moreno et al., 2020). Finally, information retention refers to the ability to recall previously encountered information, which is crucial for retaining knowledge and skills over time (Townshend et al., 2023). Among the variables of INF, retention (INF3) had the highest factor loading at 0.908, followed by interpretation (INF2) at 0.848 and exposure (INF1) at 0.721. These findings suggest that not only clear and accurate information distribution but also how individuals perceive and interpret this information are crucial in shaping COVID-19 PVT. Recognizing these factors can inform interventions aimed at fostering positive health behaviors and mitigating COVID-19 spread.
7. CONCLUSION
This research has demonstrated a significant correlation between INF and PVT in response to COVID-19 among the working-age population in Bangkok and the metropolitan area. Based on statistical analysis of the findings, all hypotheses were confirmed. The findings highlight that effective information dissemination and interpretation play a pivotal role in influencing PVT. This study underscores the importance of tailored public health messaging and interventions that take into account the cultural and contextual nuances of INF. The results advocate for ongoing efforts to provide clear, credible, and contextually relevant information to the public, thus enhancing their capacity for informed decision-making and engagement in PVT.
Based on the results, the process of INF has a positive impact on people’s preventative health behaviors. While this study was conducted in Bangkok and the metropolitan area, its findings may have broader implications for public health policy beyond Thailand. The results can be beneficial for Thai local governments and health organizations in other countries. Many countries recognize the importance of self-care for health and include it in their health literacy strategies. Consequently, these organizations should prioritize strategic health information provision, health promotion, and the dissemination of high-quality health information to the public via multiple channels. This includes providing engaging materials, making authoritative sources more accessible, and improving public engagement. Such efforts will enable people to understand essential health knowledge and apply it to promote their own and their families’ health. This approach can lower the risk of misinformation, prevent careless health practices, and potentially reduce future medical issues.
REFERENCES
, (2022) The role of digital technology in curbing COVID-19 International Journal of Environmental Research and Public Health, 19, 8287 https://doi.org/10.3390/ijerph19148287. Article Id (pmcid)
, , , , , (2020) Social media as a recruitment platform for a nationwide online survey of COVID-19 knowledge, beliefs, and practices in the United States: Methodology and feasibility analysis BMC Medical Research Methodology, 20, 116 https://doi.org/10.1186/s12874-020-01011-0. Article Id (pmcid)
, , , , , (2020) COVID-19 - Knowledge, attitude and practice among medical and non-medical university students in Jordan Journal of Pure and Applied Microbiology, 14, 17-24 https://doi.org/10.22207/JPAM.14.1.04.
, , , (2020) COVID-19 reinforces the importance of handwashing Journal of Clinical Nursing, 29, 2760-2761 https://doi.org/10.1111/jocn.15313. Article Id (pmcid)
, , , (2020) Role of mass media and public health communications in the COVID-19 pandemic Cureus, 12, e10453 https://doi.org/10.7759/cureus.10453.
(2020) Knowledge and behaviors toward COVID-19 among US residents during the early days of the pandemic: Cross-sectional online questionnaire JMIR Public Health Surveill, 6, e19161 https://doi.org/10.2196/19161. Article Id (pmcid)
(1993) What is coefficient alpha? An examination of theory and applications Journal of Applied Psychology, 78, 98-104 https://doi.org/10.1037/0021-9010.78.1.98.
, , , , , (2021) Physical exercise as a tool to help the immune system against COVID-19: An integrative review of the current literature Clinical and Experimental Medicine, 21, 15-28 https://doi.org/10.1007/s10238-020-00650-3. Article Id (pmcid)
, , , , , , , (2022) Socially vulnerable populations adoption of technology to address lifestyle changes amid COVID-19 in the US Data and Information Management, 6, 100001 https://doi.org/10.1016/j.dim.2022.100001. Article Id (pmcid)
(2022) The roles of health and e-health literacy, conspiracy beliefs and political sympathy in the adherence to preventive measures recommended during the pandemic International Journal of Environmental Research and Public Health, 19, 8346 https://doi.org/10.3390/ijerph19148346. Article Id (pmcid)
, , , , , (2020) Physical exercise as a multimodal tool for COVID-19: Could it be used as a preventive strategy? International Journal of Environmental Research and Public Health, 17, 8496 https://doi.org/10.3390/ijerph17228496. Article Id (pmcid)
, , , , , , (2021) Adherence to food hygiene and personal protection recommendations for prevention of COVID-19 Trends in Food Science & Technology, 112, 847-852 https://doi.org/10.1016/j.tifs.2021.03.016. Article Id (pmcid)
, , , (2020) Association between public knowledge about COVID-19, trust in information sources, and adherence to social distancing: Cross-sectional survey JMIR Public Health Surveill, 6, e22060 https://doi.org/10.2196/22060. Article Id (pmcid)
, , (2020) COVID-19: Prevention and control measures in community Turkish Journal of Medical Sciences, 50, 571-577 https://doi.org/10.3906/sag-2004-146. Article Id (pmcid)
(2021) Moderate exercise may prevent the development of severe forms of COVID-19, whereas high-intensity exercise may result in the opposite Medical Hypotheses, 157, 110705 https://doi.org/10.1016/j.mehy.2021.110705. Article Id (pmcid)
, , , , , (2023) Do the vaccinated perform less distancing, mask wearing and hand hygiene? A test of the risk compensation hypothesis in a representative sample during the COVID-19 pandemic Vaccine, 41, 4027-4030 https://doi.org/10.1016/j.vaccine.2022.10.028. Article Id (pmcid)
, , , (2022) Actual conditions of person-to-object contact and a proposal for prevention measures during the COVID-19 pandemic Scientific Reports, 12, 18092 https://doi.org/10.1038/s41598-022-22733-9. Article Id (pmcid)
, (2020) Assessment of health information about COVID-19 prevention on the internet: Infodemiological study JMIR Public Health Surveill, 6, e18717 https://doi.org/10.2196/18717. Article Id (pmcid)
(2022) Pandemic management requires exposure science Environment International, 169, 107470 https://doi.org/10.1016/j.envint.2022.107470. Article Id (pmcid)
, , , , , , , , , , , (2021) Effects of centralized isolation vs. home isolation on psychological distress in patients with COVID-19 Journal of Psychosomatic Research, 143, 110365 https://doi.org/10.1016/j.jpsychores.2021.110365. Article Id (pmcid)
, , , , , , , (2021) Knowledge, attitudes, practices, and the effects of COVID-19 among the youth in Kenya BMC Public Health, 21, 1020 https://doi.org/10.1186/s12889-021-11067-2. Article Id (pmcid)
, , , , , , , , , , , (2021) Beyond the pandemic: COVID-19 pandemic changed the face of life International Journal of Environmental Research and Public Health, 18, 5645 https://doi.org/10.3390%2Fijerph18115645. Article Id (pmcid)
, (2023) Everyday life information seeking in South Korea during the COVID-19 pandemic: Daily topics of information needs in social Q&A Online Information Review, 47, 414-430 https://doi.org/10.1108/OIR-10-2021-0547.
, (1970) Determining sample size for research activities Educational and Psychological Measurement, 30, 607-610 https://doi.org/10.1177/001316447003000308.
, , (2020) COVID-19 communication management in Spain: Exploring the effect of information-seeking behavior and message reception in public's evaluation https://doi.org/10.3145/epi.2020.jul.02.
National Statistical Office of Thailand (2021) Population and housing census https://www.nso.go.th/nsoweb/main/summano/aE?set_lang=en
, , (2021) Impact of information exposure on perceived risk, efficacy, and preventative behaviors at the beginning of the COVID-19 pandemic in the United States Health Communication, 36, 23-31 https://doi.org/10.1080/10410236.2020.1847446.
, , , , , , , , , , , , , , , (2022) Home-based remedies to prevent COVID-19-associated risk of infection, admission, severe disease, and death: A nested case-control study Evidence-Based Complementary and Alternative Medicine, 2022, 4559897 https://doi.org/10.1155/2022/4559897. Article Id (pmcid)
, , , (2023) Association between trust in COVID-19 information sources and engaging in infection prevention behaviors in Japan: A longitudinal study Patient Education and Counseling, 111, 107686 https://doi.org/10.1016/j.pec.2023.107686. Article Id (pmcid)
, , , (2023) Preventive behaviors and influencing factors among Thai residents in endemic areas during the highest epidemic peak of the COVID-19 outbreak International Journal of Environmental Research and Public Health, 20, 2525 https://doi.org/10.3390/ijerph20032525. Article Id (pmcid)
, , , , , , , , , , (2022) Knowledge of COVID-19 and its relationship with preventive behaviors and vaccination among adults in Northern Thailand's community International Journal of Environmental Research and Public Health, 19, 1521 https://doi.org/10.3390/ijerph19031521. Article Id (pmcid)
, , (2021) COVID-19-related knowledge, risk perception, information seeking, and adherence to preventive behaviors among undergraduate students, southern Iran Environmental Science and Pollution Research, 28, 59953-59962 https://doi.org/10.1007/s11356-021-14934-y. Article Id (pmcid)
, , , (2015) What are judgment skills in health literacy? A psycho-cognitive perspective of judgment and decision-making research Patient Preference and Adherence, 9, 1677-1686 https://doi.org/10.2147/PPA.S90207. Article Id (pmcid)
(1990) Implicit memory: Retention without remembering American Psychologist, 45, 1043-1056 https://doi.org/10.1037/0003-066X.45.9.1043.
, , , (2021) Factors associated with COVID-19 preventive health behaviors among the general public in Mexico City and the State of Mexico PLoS One, 16, e0254435 https://doi.org/10.1371/journal.pone.0254435. Article Id (pmcid)
, , (2022) Resilience during crisis and the role of age: Involuntary telework during the COVID-19 pandemic International Journal of Environmental Research and Public Health, 19, 1762 https://doi.org/10.3390%2Fijerph19031762. Article Id (pmcid)
, , , , (2021) Food safety and evaluation of intention to practice safe eating out measures during COVID-19: Cross sectional study in Indonesia and Malaysia Food Control, 125, 107920 https://doi.org/10.1016/j.foodcont.2021.107920. Article Id (pmcid)
, , , , (2022) The impact of the COVID-19 pandemic on anxiety, health literacy, and eHealth literacy in 2020 related to healthcare behavior in Thailand Journal of Public Health and Development, 20, 188-202 https://doi.org/10.55131/jphd/2022/200115.
, , , (2023) Assessment of patient retention of inpatient care information post-hospitalization The Joint Commission Journal on Quality and Patient Safety, 49, 70-78 https://doi.org/10.1016/j.jcjq.2022.11.002.
, , , , (2021) Poor sleep quality and its relationship with individual characteristics, personal experiences and mental health during the COVID-19 pandemic International Journal of Environmental Research and Public Health, 18, 6030 https://doi.org/10.3390%2Fijerph18116030. Article Id (pmcid)
World Health Organization (2020) Coronavirus disease 2019 (COVID-19): Situation report - 32 https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200221-sitrep-32-COVID-19.pdf?sf%20vrsn=4802d089_2
World Health Organization (2024) Nutrition advice for adults during the COVID-19 outbreak https://www.emro.who.int/nutrition/covid-19/nutrition-advice-for-adults-during-the-covid-19-outbreak.html
, , , , , , , , (2021) Consuming information related to COVID-19 on social media among older adults and its association with anxiety, social trust in information, and COVID-safe behaviors: Cross-sectional telephone survey Journal of Medical Internet Research, 23, e26570 https://doi.org/10.2196/26570. Article Id (pmcid)